Monday, December 23, 2013
Stroke
What is a Stroke?

A stroke or "brain attack" occurs when a blood clot blocks an artery (a blood vessel that carries blood from the heart to the body) or a blood vessel (a tube through which the blood moves through the body) breaks, interrupting blood flow to an area of the brain. When either of these things happen, brain cells begin to die and brain damage occurs.
When brain cells die during a stroke, abilities controlled by that area of the brain are lost. These abilities include speech, movement and memory. How a stroke patient is affected depends on where the stroke occurs in the brain and how much the brain is damaged.
For example, someone who has a small stroke may experience only minor problems such as weakness of an arm or leg. People who have larger strokes may be paralyzed on one side or lose their ability to speak. Some people recover completely from strokes, but more than 2/3 of survivors will have some type of disability.
Use FAST to remember the warning signs:

TAKE ACTION FOR EACH TIME WHEN ANY SYMPTOMS FIRST APPEAR. If given within three hours of the first symptom, there is an FDA-approved clot-buster medication that may reduce long-term disability for the most common type of stroke. There are also two other types of stroke treatment available that might help reduce the effects of stroke. Read more about stroke treatment.
Learn as many stroke symptoms as possible so you can recognize stroke as FAST as possible.
Stroke symptoms include:
- SUDDEN numbness or weakness of face, arm or leg - especially on one side of the body.
- SUDDEN confusion, trouble speaking or understanding.
- SUDDEN trouble seeing in one or both eyes.
- SUDDEN trouble walking, dizziness, loss of balance or coordination.
- SUDDEN severe headache with no known cause.
- THE END -
Sunday, December 22, 2013
Exercise
EXERCISE OF OCCUPATIONAL THERAPY FOR
STROKE PATIENTS
Scapular Mobilization
Passive Range of Motion
Rowing
Tapping
Weightbearing
Heavy Joint Compression
Light Stroking
-THE END-
ADL Training
General Tips for Dressing
- When dressing, always put clothing on the affected side first. When undressing, always take clothes off the affected side last.
- Clothing that must be pulled over the head (undershirts, nightgowns, sweaters) may be difficult to manage.
- When getting dressed, lay out clothes in the order they will be put on. Those to be put on first go on top of the pile.
- Putting on clothes is easier when sitting than when lying down.
- Let's us go on detail on how dressing techniques are used for stroke patients.
a) A Pullover Garment


b) Donning a shirt



c) Donning A Pant



d) Socks



e) Lacing Shoelace



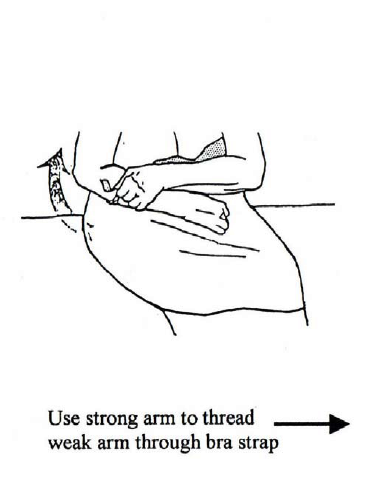
f) Donning A Bra



Tips for Bathing
- From dressing, let go through how to do a bathing technique....

- THE END -
What Is OT??
Firstly, let's us watch together a video about what is an OCCUPATIONAL THERAPY?
enjoy!!
so??
what is an OCCUPATIONAL THERAPY?

Occupational Therapy is a therapy based on engagement in meaningful
activities of daily life. Occupational therapy helps to solve the problems that
interfere with your ability to do the things that are important to you. It can
also prevent a problem or minimize its effects.
When an injury,
illness, disability or other problem limits your ability to:
• Take care of
yourself,
• Participate in paid or unpaid work, or
• Enjoy your leisure time, e.g. hobbies, sports, spending time with family,
• Participate in paid or unpaid work, or
• Enjoy your leisure time, e.g. hobbies, sports, spending time with family,
then you may want to
learn some new skills for the job of living from an
occupational therapist.
Occupational
therapists believe that occupations (activities) describe who you are and how
you feel about yourself. If you are unable to do the things you want, or need
to do, to live and enjoy your life, your general well-being may be affected.
Occupational Therapy
in Stroke can help
you develop your skills and confidence to manage activities that are
important to your health and well-being. After your stroke you
may be facing a range of difficulties that make it hard for you to
do the things you would like. These difficulties can include physical
problems, difficulties with your memory or attention, problems with
your vision or sensation and emotional problems such as anxiety or
depression (low mood).
Your occupational
therapist will work with you to find ways of overcoming any
difficulties. They might give you exercises to practice, help
you find new ways of doing things or suggest equipment that could
help. Your therapist will help you set goals which will often be
broken down into smaller, more manageable tasks. Your goal may be to
walk to the local shop but you might start by walking to the front
door, then down the path and so on, gradually building your confidence and
abilities.
Depending on your
needs, an occupational therapist may:
•• assess your
difficulties and explain them to you and your family
•• suggest activities
to improve your abilities and independence
•• use and adapt
everyday activities as part
of your rehabilitation
•• teach you strategies
and techniques to overcome any remaining difficulties
•• provide aids and
equipment
•• visit your home to
check that it is suitable for you
•• advise on the best
way and the best time for you to return to work, which may include
talking to your employer (with your permission) about how they
can support you
•• support your carers to be able to
look after you.

Transfering Technique
TRANSFER
Moving From Bed to Chair or Chair to Toilet
Safely helping a survivor to move depends on the abilities of both the health care provider and the survivor. No single technique works in all situations. Consider the following factors when planning a transfer:
• The survivor’s level of control and movement: Poor control of the affected side may cause
overuse of the unaffected side during transfers.
• Size and weight of the survivor compared with the health care provider.
• Time of day and how tired the survivor is (a fatigued survivor needs more help). Is the survivor
better able to perform in the morning but fatigued at night?.
• Your level of comfort in safely moving the survivor. If you are not sure you can do this safely,
ask for help.
Rules For Safe Transfers
Follow these steps when helping a stroke survivor to move:
1. Make sure the survivor is wearing safe shoes.
2. Apply wheelchair brakes.
3. Move any arm rests and swing foot rests out of the way. Support the affected arm with a sling
if needed.
4. Help the survivor get into the right starting position. The persons unaffected side should be closest to the chair. Shift the person’s buttocks closer to the edge of the wheelchair, one side at a time.
5. Position yourself as close to the survivor as possible. Do not block the direction of movement or the survivor’s view of the path of movement.
6. Guide and support the survivor’s upper body. Place your hands around the upper back and
shoulder blades.
7. Bend your knees and keep your back straight. Note: Do not lift the survivor by placing your hands under the arms or armpits. This can cause pain. Do not pull the affected arm.
8. Shift your weight from the front to the back foot. Doing this makes the transfer easier.
One-Person Pivot (Stepping) Transfer
A one-person pivot (stepping) transfer is often used for assisting a survivor to stand. It is also used for
toilet, car, and bed-to-wheelchair transfers.
Follow these steps:
1. Stand in front of the survivor, supporting the shoulder blades.
2. Tell the survivor which way they are being moved.
3. Rock the survivor gently forward and guide the person to a standing position.
4. Position your feet on either side of the affected foot to support the leg and prevent it
from collapsing.
5. Assist survivor to step and transfer weight to the leg closest to the destination.
6. Pivot.
7. Help the survivor bend forward and place the buttocks down and back on the new surface.
Two-Person Pivot (Stepping) Transfer
The two-person pivot (stepping) transfer is used on the survivor who can bear weight on the legs but is heavy, likely to make sudden movements, or unable to follow direction. You need 2 health care providers for this transfer. The taller care provider stands behind the survivor. The care provider at the front leads the transfer. The rear care provider guides the hips.
Step 1: Getting ready for the transfer
A. Both caregivers:
• Lower the bed so the survivor’s feet rest on the floor.
• Lock the bed brakes, if the bed has casters.
• Adjust or remove the wheelchair foot rests and the arm rest on the side closest to the bed.
• Place the wheelchair beside the bed at a slight angle.
• Lock the wheelchair brakes to allow the rear care provider to be closer to the survivor.
B. If you are standing in front:
• Assist the survivor to sit on the edge of the bed with feet flat on the floor.
• Have the survivor place the unaffected arm around your waist.
• Place your hands on the survivor’s upper back.
• Position your feet on either side of the affected foot to support the leg and prevent it from collapsing.
C. If you are standing behind:
• Stand behind the survivor with one knee on the bed.
Step 2: The transfer
A. If you are standing in front:
• Use a no-verbal signal (like a head nod to the second caregiver) to start the transfer if the survivor overuse their unaffected side.
• Assist the survivor to transfer weight to the leg closest to the destination.
• Turn, and place the buttocks down and back on the new surface. Note: A transfer belt placed low on the survivor’s pelvis can simplify this step. It can also make it more comfortable for the survivor, and allow the care provider at the back to help more.
B. If you are standing behind:
• S upport the survivor at hip level and guide (do not lift) the hips.
C. Both caregivers:
• Do not lift using the survivor’s clothing
• Replace the wheelchair foot rests and arm rest
• Position the survivor comfortably
A low-pivot transfer may be more effective if the stroke survivor can help by coming into a half-standing
position, but not a full standing position. Follow the steps above.
Wheelchair Use
Even after treatment, most survivors have some problems moving. These problems range from someone who is easily fatigued to being unable to move. A survivor may require a wheelchair for part or all of the day. The physiotherapist or occupational therapist can decide what wheelchair is needed. They will know whether or not the survivor will also need a pressure-relieving cushion and back support. Many survivors learn to move their wheelchair during rehabilitation. You may need to remind them how best to use their wheelchair.
Survivors may slide forward in a wheelchair so that their feet can reach the floor. Sliding forward in a wheelchair can:
• Affect postural tone and control
• Cause problems with transfers and control
• Increase high tone (spasticity), pain, and the risk of skin breakdown
The physiotherapist or occupational therapist may prescribe a hemi-height wheelchair. This chair has a lower seat than a standard chair. It allows the survivor to reach the floor with their feet without sliding forward.
What You Can Do to Help?
Watch the survivor moving the wheelchair so you can spot any problems. Ask yourself these questions:
• Does the movement look normal? If not, why not?
• What can I do to change it?
• Do I need to have a member of the team assess the survivor?
Watch for increasing muscle tone (stiffness). This tells you that the survivor is using too much effort. Check with the healthcare team if you are concerned. Excessive effort reinforces abnormal movements. Make sure the survivor is not doing too much too soon.
The Too Much, Too Soon Rule!!
Doing too much, too soon has a long-term, negative effect on the survivor’s ability. Overuse can cause wear and tear on the unaffected side and increase the need for help. Always balance the benefits of faster independence with the risk of overuse and deterioration.
- THE END -
Adaptation Devices
- Adaptive devices is used to compensate for physical limitation, to promote safety, and to prevent joint injury.
- Adaptive devices also will help client to be independent in their occupational performance.
- Before recommending an adaptive equipment, OT practitioner must complete a through assessment to determine the client’s functional problems and cause of the problems.
Shoehorn

This devices will help in put on shoe by keeping the shoe open and by providing a smooth surface for the foot and heel to move.
Dressing Stick or Reacher

Its can be used to push a shirt/blouse over the head. It is also for pushing and pulling garment off and on feet and legs.
Buttonhook/Zipper
.jpg)
It will help the client to buttoning/zip their cloth easier. Another alternative is to replace the button with bigger button or Velcro.
Sock Aid

Extended-Handle Reacher

It is used to pick up socks and shoes, arranging clothes, removing clothes from hangers, pick up objects on the floor and donning pants.
Swivel Spoon

Plate With Plate Guard

Utensil Holders and Universal Cuffs

It is for person that had limited grip or dexterity but have good control of shoulder and elbow. There are also weighted cuff that is used to decrease involuntary motion and compensate for incoordination.
Cutting Board with Stainless Steel Nails

It is to stabilize the meats and vegetable while cutting. it is useful for patients with incoordination or use one hand. Bottom of the board should have suction cup so that the board does not move.
- THE END -
Monday, December 2, 2013
Socks Aid Administration



{kind=link}
{kind=link}
Subscribe to:
Posts
(Atom)